[[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello, and welcome back to “What The Health?” I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Thursday, November 14th, at 10 a.m. As always, and particularly this week, news happens fast and things might’ve changed by the time you hear this. So, here we go.
Today we are joined via videoconference by Rachel Roubein of The Washington Post.
Rachel Roubein: Hi. Thanks for having me.
Rovner: Anna Edney of Bloomberg News.
Anna Edney: Hello.
Rovner: And Lauren Weber, also The Washington Post.
Lauren Weber: Double trouble today. Thanks for having me.
Rovner: No interview this week but more than enough news to make up for it, so let’s dig right in. So as of yesterday, it’s official. Come January 20th, Republicans will control the presidency, the Senate, and the House, although the final split is still yet to be determined and might be even smaller than the handful it is now. Plus President-elect [Donald] Trump keeps naming House Republicans to his administration, which will complicate things and which we’ll talk about in a moment. But assuming there is a trifecta when Trump puts his hand on the Bible at noon on January 20th, what difference is that going to make to the health agenda than if the House had flipped Democratic, even by a vote or two?
Edney: Well, I think that, as you just mentioned, this majority is likely to be so small. And just thinking to the past, we’ve seen such divisions, even among the Republican Party, on what should be done.
Rovner: It only takes one or two — when you can only afford to lose one or two votes, it only takes one or two people to gum up the works.
Edney: Yeah, and there are a lot of members — and particularly, it seems like, in the GOP — that are very willing to do that. I mean, I think that also the potential is that health care is not top of mind for President Trump, at least. So I know we’ve heard Speaker [Mike] Johnson say that he would like to overturn the ACA [Affordable Care Act] right away, but I don’t know that, like we said, with the small majority, that that will be able to even happen.
Rovner: I feel like that’s a big difference from, I would say from 2017, when we came in and health care, repealing ACA, was right at the top. Not so much now. Lauren.
Weber: I was just going to say: What version of the Trump administration on health care are we going to get? I mean, you have Robert F. Kennedy Jr. out there talking about “Make America Healthy Again,” which also flies in the face of a lot of Republican ideology. I mean, a lot of what he’s talking about seems to be high regulation of ultra-processed foods. He seems to want to limit advertising for pharmaceutical ads. He wants to focus on chronic disease, which is something that a lot of people on the left would love to see more interest in, along with the ultra-processed food. But is that the new Republican Party focus for health? I don’t know. I think we’re going to see, I mean, considering RFK seems poised for a large position in the administration.
Rovner: And we’ll talk more about him in a few minutes. Rachel, you wanted to add something.
Roubein: Yeah. I think of — when I think about Congress and the power structure, I’m thinking a lot about just the government spending bills and how that is used to negotiate. Like, if you look from a few years ago, Democrats negotiated some Medicaid policies that they wanted on maternal health for exchange for what Republicans wanted on unwinding Medicaid. And so Democrats lose their negotiating leverage there. And really one of the big policies in Congress for next year, I think, is the expiration in 2025 of the enhanced Obamacare subsidies. So Democrats don’t really have a chamber there.
Rovner: Which we’ll also get to. But, I mean, the big difference is that if the Democrats had gained a majority even by one or two votes, that would’ve given them control of committees, which now they won’t have. And that is, yes, a big deal. I was going to say, Anna, in a year when health is not necessarily at the top of the sort of big agenda, what happens in committee is often what happens.
Edney: Right, yeah, what they decide to look into or not to look into. One of the places maybe where they could sort of cross paths or agree in a way with RFK Jr., if that’s the way the Trump administration goes, is there’s still a lot of anger on the right about the covid vaccine. So we could see investigations ongoing — I think they’re still happening — but ongoing in that vein, and [Anthony] Fauci could keep getting called before Congress. And that leads to a sort of aversion to pandemic preparedness, which could be concerning because we’re looking down at this bird flu potential problem that keeps getting slightly more concerning all the time.
Rovner: There’s a teenager in Canada in intensive care with bird flu, who was not exposed to anything on a farm. That has public health people concerned.
Edney: Right, right, exactly. And when you think about raw milk and RFK Jr. in support of that — I know we’ll get to him — but it all feels like a perfect storm, potentially. But I think that the way that the Republicans would prefer to go is not dealing with — they’d rather gut pandemic preparedness. They don’t see a place for it, so that those things could become important down the line.
Rovner: So as I mentioned, President-elect Trump is already announcing lots and lots of people to staff the upper levels of his incoming administration. And even with the Senate, with the Republican majority, that seems pretty likely to give him whatever he wants, he’s been curiously suggesting that he wants to use something called recess appointments for his major offices, which would mean his appointees would be temporary, but they would also avoid the normal Senate confirmation process, which involves vetting and hearings and votes and even on an expedited basis can take weeks. Are we starting to get an idea of why he wants that, given some of the folks that he’s already named, like firebrand and ethics-challenged Republican congressman Matt Gaetz to be attorney general?
Edney: Yeah, certainly. We haven’t seen an HHS [Department of Health and Human Services] pick yet, and I can’t even guess who it might be just given what’s already come out was very unexpected. And so I think that you’ve seen agencies like the Food and Drug Administration go through that before, where they’ve just had these temporary people or they’ve kept in place whoever was the deputy at the time, and they become the commissioner for a while and not confirmed. And it really hampers their ability to do a lot, though. There are decisions that a department or an agency can’t make if someone’s not Senate-confirmed.
Rovner: But doesn’t that throw more power back to the White House? Isn’t that kind of the idea here?
Edney: Yeah, true. That’s a good point. If RFK Jr. gets this sort of health czar spot — I’ve been telling people I couldn’t really see him as HHS secretary, because a lot of what he wants to do is under the USDA [Agriculture Department]so that would make no sense. And so if he just kind of has the power he wants in the White House to do what he needs, you make a good point there as well.
Rovner: Yeah, what else are — I would’ve said before yesterday that they would never name RFK Jr. to be HHS secretary. Although after some of the names we got yesterday, maybe that will happen. This could happen while we’re taping this. But what other names are we hearing, if any? I know I have three people here who have been covering the FDA. I mean, obviously during the first Trump administration, the FDA was headed by Scott Gottlieb, who we would consider a traditional Republican, a doctor. He’d worked in the agency before. He’d been in government. That doesn’t seem likely what we’re going to see this time around.
Edney: I think that’s true. I think the one thing is what Trump’s focus will be. If he does let someone else kind of take the reins on this, maybe we would see someone a little more measured. I would say right now, most of the names that I’m hearing for HHS or FDA are very much recycling from last time around. And so I’m really unsure whether people are just batting that around because those are names that have come forward before or whether that’s who we’ll actually see named. I think we will know in short order, because I do think that these are coming out quickly. And I appreciated, Julie, that you corrected everyone that they’re not nominated. There is an intent to nominate by a president-elect, so, but still will—
Rovner: Although, I will say, his statements say that he’s nominating, which is confusing people.
Edney: Yeah. I think they’re less concerned with the specifics.
Rovner: Yes. Well, surprise, surprise. All right, now let’s talk about RFK Jr. Obviously, we don’t know what position he’s going to fill, but we’ve talked a lot about his more Republican-friendly positions, anti-vax stuff and raw milk and sort of anti-public-health. But Rachel and Lauren, you’ve got a story up today about some other positions that Democrats might be a little more sympathetic to. What are some of those?
Roubein: There’s at least two ideas that we had sort of looked at in this story that have found some public support on both the right and the left, such as stripping ultra-processed food from school cafeterias and kind of cracking down on food dyes. And, I mean, one of the things we noted up top is that this is, some of this would be a contradiction from Trump’s first term, where Sonny Perdue, who was Trump’s agriculture secretary, within the first week or two of him being in his position, he vowed to quote-unquote “make school meals great again” and then kind of waged this assault on Michelle Obama’s efforts to make school meals healthier. That’s not to say that Kennedy being a position of power doesn’t alarm federal health officials or public health experts or people in the food industry, because it does. But there are some policies that he could have a [Sen.] Bernie Sanders agree with him on.
Rovner: And while we’re on the subject of ultra-processed food, Lauren, you’re our Lunchables correspondent, and there’s Lunchables news this week. Tell us about it.
Weber: There is Lunchables news this week, and loyal listeners of the pod will remember that I did a story at The Washington Post last year with some of my colleagues that looked at how Lunchables had ended up on school lunch trays for the first time ever. Kraft Heinz had kind of tinkered with the formula, reformulated it, and actually ended up adding more sodium while adding more protein and other things to qualify for the National School Lunch Program. And, obviously, a lot of nutrition experts were appalled because they felt like this is an example of ultra-processed foods that’s being served as free and reduced lunch to kids who don’t necessarily have as much of a choice there on what’s being served to them. And we got news this week that Kraft Heinz didn’t make enough money, that school districts did not purchase their reformulated product, and they had, due to quote “lack of demand,” they’re taking them off the options.
So it’s kind of interesting. RFK’s push against ultra-processed food is coming at a moment not just in school lunches but in the United States, where there has been growing awareness about ultra-processed foods making up 60% of the American’s diet. And for a very, very long time, food industry h as been really successful in Congress at watering down some of the regulations against stuff like ultra-processed food, especially in school lunches, to kind of weaken these regulations, as Rachel talked about, that Michelle Obama had pushed for and other ways, so that they could continue selling their products. And so some of the food industry folks that Rachel and I talked to are quite concerned about a possible RFK role because he’s really pushing against the powers that be there. And it’s really interesting to see that dynamic, because, as Rachel pointed out, the only other person that’s really been doing that recently is Bernie Sanders. So you kind of have this horseshoe of right and left that’s coming to the forefront here.
Edney: I was just going to add, I actually wrote my newsletter on this today. The FDA is doing some things in this vein that are sort of interesting. I said it was kind of an RFK-FDA, very tiny, very small Venn diagram in that the agency is also looking at ultra-processed food. They said — Jim Jones is their deputy commissioner for human foods, and he said recently that they were doing some work trying to figure out how to study whether there’s really causality, but he did say they’ve been working and they have done a lot on certain trans fats, getting them out of food. They’ve done a lot to try to, they’re trying to reduce sodium levels. That’s going to be a stepwise process in food. And they have made consumers a lot more aware, including on the label, of added sugars. And he was like, This is all what we see in processed foods that is a problem.
And so there’s sort of this quiet— they’re quietly going after it, just not calling it that. And then on the dyes, they’re certainly not going as far as RFK Jr. and saying, We want to ban all dyes. But they have had a petition in front of them for a couple years, and Jim Jones said he expected a response from the FDA. I forget exactly the quote, but it was very soon on what they’re going to do on Red Dye Number 3, which is sort of the one that has been studied the most and has links to cancer and potentially hyperactivity in kids.
Roubein: I think it’s also worth noting, in talking about the FDA’s nutrition department, is the day after the election, RFK Jr. was on MSNBC saying that there are entire departments at FDA that have to go, and he specifically said the nutrition department. Again, whether you could just have kind of a mass firing of civil servants is kind of pretty TBD, but that’s how he’s viewing the nutritionists there, and that is alarming to staff. FDA Commissioner Robert Califf the other day said that, called them hardworking people. He was asked about it and had a bit of a defense there.
Weber: Just to add in on that, too, there are some nutrition advocates that wouldn’t be that sad about that. I mean, I know that they feel like the FDA has been too slow, is too influenced by industry. I mean, look at the food label story that we talked about also on this podcast, that Rachel and I did. The Biden administration was supposed to propose potential front-of-pack labels for front of food, and a lot of nutrition advocates thought, even though this proposal has not come out yet, that what they were thinking about was too weak and too deferential to industry. So RFK has certainly tapped into this growing anger, it seems, at the lack of protections for kids or in general about the food supply. I think part of it is is that he and Trump are very good marketers. They have these catchy slogans, “Make America Healthy Again.” I think that’s somewhat at play as well.
Rovner: I think before we leave this sort of next administration segment, though, I do want to broaden it out a little bit, because we’ve been talking about this contradiction that is Donald Trump, which is, on the one hand, he’s got a group of people that wants to strip the federal government of all of its ability to regulate and get rid of regulations and let industry run wild because, as Vivek Ramaswamy says, regulation is a yoke around the neck of innovation. On the other hand, he’s got people like RFK Jr. who want to come in and say: No, let’s get industry out of government. Let government do its job regulating. I mean, the health industry must be — their heads must be spinning, because this obviously is going to affect different portions of the industry different ways, right?
Edney: Yeah, it’s a confusing thing, too, when you think about the pharma industry, for instance. I can say, they are highly regulated in the sense that they pay lots of money to the FDA, millions and millions of dollars to have their new drug applications reviewed. There’s a very strict process of what they get for that, what the FDA will do for that. They don’t want that thrown away, because that gives them a lot of security on, Here’s how things are going to work and we need to know thatversus if you just had somebody up there being like, Yes to that one, no to that one. And there could be other areas. Certainly Big Pharma would not love it if everything was tried to be cured with ivermectin and the hydroxychloroquine. So that would be a problem for all of us. So I think that there’s just a lot of confusion and uncertainty in pharma, at least.
Rovner: And I mean, the one thing we know is that industry hates uncertainty. They would like to be able to plan.
Edney: Yes. Right, yes. They very much need that for themselves, for their researchers, for their shareholders. That’s super important.
Rovner: Yeah, so obviously, everybody in health care is sort of watching eagerly. All right, well, while we’ve all been busy talking about the election, open enrollment began for the Affordable Care Act for 2025, possibly the last year that millions of Americans will remain eligible for expanded subsidies, since a fully Republican Congress and president seem unlikely to extend them beyond December 31st, 2025. What is going to become of the ACA expanded subsidies? Is there any chance they get extended? It would displace millions of people who have gotten health insurance through the ACA.
Edney: Well, I think if we’re talking in ways that Trump may be interested in, the insurance companies wouldn’t like it, because they don’t want to lose all of those patients. So I guess maybe that is the potential glimmer of hope for people who want those expanded subsidies to stay intact.
Rovner: And we still don’t know what the Republicans have in mind for the Affordable Care Act. As I like to point out, they’ve been talking about a replacement since 2010 and we’ve never actually seen one.
Roubein: Trump has concepts of a plan, he says.
Rovner: So we have heard.
Roubein: Remember that in the debate? I mean, we heard that for how many years, right? Years and years.
Rovner: Two weeks. He’s going to have something in two weeks.
Edney: I was going to say, if anyone writes an In two weeks it’s coming story, they have to buy drinks for everyone.
Rovner: Absolutely. Lauren, you wanted to say something.
Weber: I mean, I was just going to say that the first Trump administration was not known for expanding any sort of subsidies for the ACA. So I’m curious. But as Anna pointed out, frankly it’s always hard to take away something that’s popular. You don’t necessarily want those people mad at you. So to be quite honest, let’s wait and see.
Rovner: Yeah, TBD.
Weber: TBD.
Rovner: Well, this is also the first year that DACA [Deferred Action for Childhood Arrivals] recipients, the so-called “Dreamers” who were brought to the U.S. without documentation as children, are eligible themselves for subsidized ACA coverage. That’s estimated to be about 100,000 people. I wouldn’t expect that to last either, though. And I’m wondering, it might not even make it through the year, as it’s the subject of a lawsuit brought by Republican attorneys general that I expect a new Justice Department would just drop?
Roubein: Yeah, I feel like with everything, there’s kind of a road map to look at what Trump did in the first term, just kind of speaking broadly, not just on DACA. But then there are things that they might not do again. So I feel like it’s hard to predict, but yeah, feasibly I feel like that could sort of be the thinking.
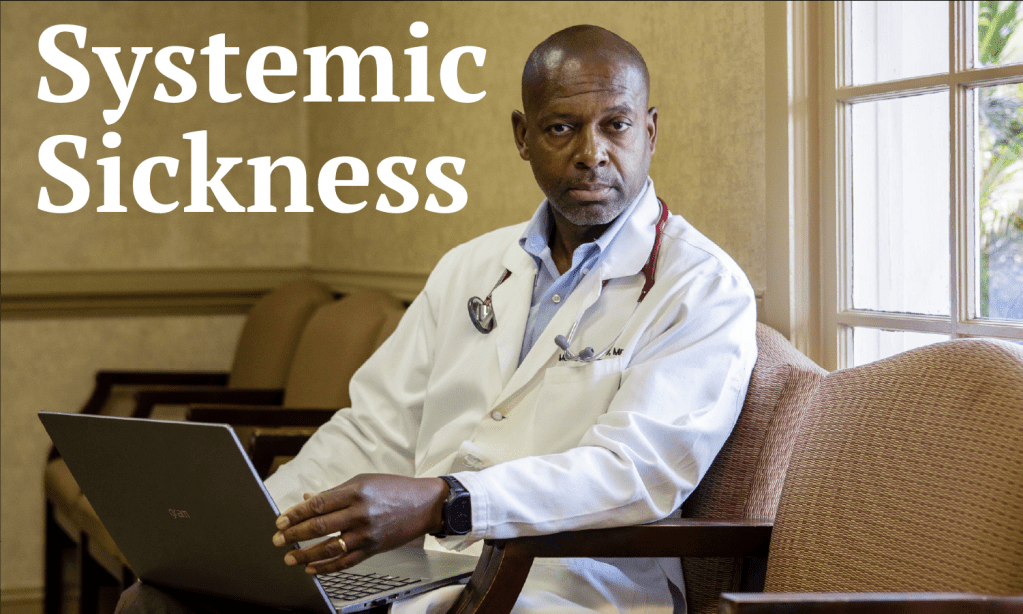
Rovner: Trump has been nothing more than unpredictable all the way through. So I’m going to do my extra-credit story early this week because I want us all to talk about it a little bit. It’s from my KFF Health News colleague Phil Galewitz, and it’s called “In Vermont, Where Almost Everyone Has Insurance, Many Can’t Find or Afford Care.” And it’s about a problem that’s kind of been sneaking up on us and is now here for all to see: Having insurance is necessary but not sufficient to get health care.
As Phil points out, Vermont has basically the lowest uninsured rate in the United States, but care there is expensive. Both providers and insurers are having financial difficulties, and growing numbers of patients either can’t find care or can’t pay for it or both. Some of this appears to be demographics. Vermont is, on average, older and more rural than most other states, and some of it is possibly due to health provider consolidation. But I feel like this is kind of the early warning of the same sorts of things happening around the country. At what point do we have to actually take stock of the fact that our health system is not functioning very well? I mean, we’re so busy talking about what industry wants and what government wants and what will help this group and what will help that group. And it’s like, even with an all-time-low uninsured rate, the stories about people being unable to get care are becoming more than anecdotal, right?
Weber: I mean, I think, Julie, go back to the name of this podcast. The podcast is called “What the Health?” I mean, I think you’ve, obviously, and all of us here have been covering this for many years. But Phil’s story was just beautifully done, because it showed how multifaceted the problem is. But that also means there’s not a quick fix. But the bottom-line kicker was these people are paying a ton of money for their health care and are having to wait months and months and months for stuff they feel like is not that great, or they’re forced to go across state lines and pay more somewhere else to get it quicker. And obviously that’s, as you said, not quite a solution. So a fascinating look at, what it seems like, a large number of factors that are causing serious issues with people’s health care delivery.
Rovner: I just feel like it’s a warning to not — I mean, obviously we are health reporters. We look at things in the micro. But sometimes I feel like we’re kind of losing the forest for the trees, and this was a really good reminder. It’s like there’s a forest out there and things are not going great in the forest.
All right, well, let’s turn to abortion. Even though seven out of 10 states with ballot measures voted for the abortion rights position — eight states, if you count Florida, where the measure to overturn the state six-week ban got 57%, but that was short of the 60% it needed to pass — the anti-abortion movement is nonetheless gearing up to undo as much of this as it can.
According to our podcast panelist Alice Ollstein, some of the strategies anti-abortion groups plan to pursue are ones that we have talked about here before, including requiring that abortion pills be labeled as a controlled substance, like they’re doing in Louisiana, or that the remains of medication abortion be handled as medical waste. Other ideas are new or at least new-ish, like trying to cut off funding to colleges and universities that provide abortion pills at campus facilities. The anti-abortion movement is also trying to push state legislation aimed at circumventing the protective amendments that tho se states’ voters just passed. This fight is a long way from being over, right?
Edney: Oh, yeah. And you just mentioned states. That’s where I’m sure that a lot of the focus is, because if Trump holds to his word, and I don’t know if that’s the case, he said it should be up to the states on how they handle all of this stuff. So I imagine now is their moment if they’re going to try some of these more out-of-the-box ways of dealing with it.
Roubein: And I think one thing that emerged, particularly after Republicans took back the House in 2022 and Roe v. Wade was overturned, was that the battleground being states, but also the executive branch. The battleground in terms of Congress, the House didn’t bring up a bill to ban abortion at 15 weeks or anything politically—
Rovner: They couldn’t have gotten the votes with their tiny majority.
Roubein: Yeah, it’s very politically tricky. We’ve seen Republicans back away from those stances. And then you look at the Biden administration, which has said, There are things we can do to sort of do some guidelines, et cetera, like letting the VA [Department of Veterans Affairs] do abortions in certain instances, or they rolled back Trump’s changes on the Title X federal family program that basically forced Planned Parenthood out. So you could sort of see some of those things being rolled back again.
Rovner: Well, one of the things that I haven’t seen noted by anybody, and I absolutely agree with you about: The first thing that the Trump and whoever in the Trump administration to do is reverse the things that [President Joe] Biden did, which in some ways were reversals of things that Trump did the first time around. But we do have a bunch of abortion-related lawsuits still in play that involve the Justice Department. Remember that Supreme Court case where the justices ruled that the anti-abortion doctors who brought the case didn’t have standing to sue? Well, that case is still alive. It’s still in court, because states have stepped in as plaintiffs. Then there are cases challenging the Biden administration’s interpretation of EMTALA, which is the federal law that requires emergency abortions be provided to protect a pregnant woman’s health and says that those override state laws that only allow abortions if the woman’s life is imminently endangered. I would think those cases would go away under Attorney General Matt Gaetz or whoever is going to be in charge of the Justice Department, right?
Edney: I mean, that makes perfect sense to me that they would not continue arguing those by any means unless Trump is more focused on trying to overturn his own convictions. I don’t know what that could look like.
Rovner: Yes, no matter what, the Justice Department will be very busy, but I suspect not very busy arguing the abortion rights side of abortion cases.
Edney: Right.
Rovner: Well, I want to turn to Medicare. Trump insisted during the campaign that he wouldn’t touch Medicare, but that’s not actually possible for a Congress and an administration. The only real question is how Medicare will be touched. Doctors are, once again, facing a Medicare pay cut for next year. This one is just under 3%. And that’s something that the lame-duck Congress, which is just getting back into session this week, may or may not cancel, given how crazy things are right now on Capitol Hill. And The Wall Street Journal has a piece this week about how sicker people are leaving their Medicare Advantage plans to return to traditional Medicare, which makes sense because private Medicare Advantage plans make care harder to access when you’re sick. So that ends up making — when they leave, it ends up making the plans richer because they don’t have to pay for the care, and the taxpayers poorer because now Medicare, traditional Medicare, is paying for the care. So Medicare’s going to have to be on the table in some form. We can’t just ignore Medicare for four years, right?
Edney: Yeah, I think particularly this is the sort of bigger picture. But when you think about if Trump does want to do a bunch of tax cuts and where does the money come from, I’m sure there are ways to do it. There are all kinds of budget tricks that can be done to look like you’re not touching Medicare but you’re touching Medicare, so you can keep that campaign promise. And I don’t know if that’s really on the table for them, but I don’t think we can expect no one to be looking at this, particularly also because of the sort of Republican desire to prop up the Medicare Advantage a little bit more to get … So I don’t know if there’s a way to encourage some people back on those plans or how they’re going to look at that.
Rovner: Yeah, it’s important to remember that the traditional Republican idea on Medicare is to get more people to go into Medicare Advantage, which is happening naturally anyway because people who are aging into Medicare are mostly coming out of managed care plans, so they’re used to being in managed care plans. So it’s easy for them to go into these Medicare Advantage plans that say, Hey, we’re going to offer you extra benefits that Medicare doesn’t. And it’s not until they actually need care and can’t get it that they realize that maybe that wasn’t the best idea. But I certainly expect this entire debate to carry over to the next administration.
Edney: Well, and you also … I don’t know why, but you reminded me that there are still drugs to negotiate under Medicare.
Rovner: That’s right.
Edney: And you somehow have to deal with that, and taking it away would be pretty difficult, seemingly.
Rovner: And cost a lot of money.
Edney: And cost a lot of money. But you could negotiate things differently or — I’m not sure.
Rovner: Yes, we’ll have plenty of Medicare to talk about. All right, well, that is the news, at least up until this moment. Now it’s time for our extra-credit segment. That’s where we each recognize a story we read this week we think you should read, too. Don’t worry if you miss it. We will put the links in our show notes on your phone or other mobile device. I’ve already done mine. Anna, why don’t you go next? Yours is so very on brand for you.
Edney: Thank you. So mine is from The Atlantic. It’s called “Throw Out Your Black Plastic Spatula.” Certainly, I grew up in my family and my parents still have all their black cooking utensils. And what this is talking about is how most of our black cooking utensils are made from recycled electronics. And there’s a whole reason for that. It’s really interesting to read about. But the outcome is that there are also a lot of fire retardants in those, so we are getting fire retardants leaching out into our food.
Rovner: Of course, fire retardants are why they had them in the first place, right? Because you’re putting them in very hot things.
Edney: Well, this is more because of the electronics. Like, yeah, when you’re using an electronic, I guess there’s fire retardants in there because you don’t want the battery blowing up or whatever. But if you’re recycling those and making utensils out of them, then you’re going to get some of that in your food.
Rovner: The dark side of recycling.
Edney: Yes.
Rovner: Lauren, why don’t you go next?
Weber: Mine’s actually a study in JAMA that’s titled “Medical Board Discipline of Physicians for Spreading Medical Misinformation.” And the study found that actually the least common reason for medical board discipline was spreading misinformation, which was not actually news to me or some of my colleagues at The Washington Post, as they cite our work in this study. But Lena Sun, Hayden Godfrey, and I last year did a large investigation in which we actually surveyed all 50 medical boards and went through and asked them about whether or not they had disciplined anyone for misinformation.
And then on the boards that did not respond, which was many, we then went through and read every single disciplinary action to see what we could find. And the bottom line is is doctors didn’t get punished. There’s a lot of free-speech protections, and, frankly, it had to be very, very, very egregious for medical boards to step in. In general, medical boards are weak. They are known to be poor at self-regulating their own. It takes a lot to really get punished by a medical board, so it’s not that surprising. But after a lot of clamor during covid and a lot of physicians that really became megaphones for unscientific evidence, it’s still quite striking that not very many of them faced any sort of repercussions for that.
Rovner: Yeah, another issue going forward. Rachel.
Roubein: My extra credit, it’s titled “‘Been a Long Time Since I Felt That Way’: Sexually Transmitted Infection Numbers Provide New Hope,” in Politico by Alice Miranda Ollstein. The story talks about basically how there’s been this drop in sexually transmitted infections, and that has followed years of just skyrocketing cases. So this is from new data from the Centers for Disease Control and Prevention that came out this week. So, for instance, total cases of syphilis increased 1% and congenital syphilis ticked up 3%, but that’s a far slower rate of growth than the spikes of the last few years. So that’s an encouraging note for STD health directors in states. But in the piece, she talks about how there’s some concern from public health experts and other advocates about potentially backsliding under Trump, depending what happens, and also noting that Congress last year clawed back hundreds of millions of dollars in public health funding.
Rovner: That’s right. And obviously the federal Family Planning Program plays a big role in the prevention of sexually transmitted infections, and we have no idea what’s going to become of the federal Family Planning Program under a Republican trifecta. So again, a story that I’m sure we will spend more time talking about.
All right, that is this week’s show. As always, if you enjoy the podcast, you can subscribe wherever you get your podcasts. We’d appreciate it if you left us a review. That helps other people find us, too. Special thanks this week to our temporary production team, Taylor Cook and Lonnie Ro, as well as our editor, Emmarie Huetteman. As always, you can email us your comments or questions. We’re at whatthehealth, all one word, @kff.org. Or you can still find me at X @jrovner and increasingly at Bluesky @julierovner.bsky.social. Where are you guys these days? Lauren?
Weber: Still just on X, LaurenWeberHP. The “HP” is for “health policy.”
Rovner: Anna.
Edney: On X. It’s @annaedney. And I am trying out Bluesky as well, but I’m so new that I don’t even remember my name.
Rovner: It’s OK.
Edney: I’ll get that next time.
Rovner: Rachel.
Roubein: Similarly to Lauren, on X, @rachel_roubein.
Rovner: We will be back in your feed next week. Until then, be healthy.










You must be logged in to post a comment.